
Why Single Payer?
The short answer is that single payer is the most equitable and affordable option for the design of a universal system, and the more comprehensive the single payer system is, the more equitable and affordable health care becomes.
What are the options For A Universal System?
Our mission is to bring about equitable, affordable, comprehensive, high quality, publicly-funded health care to everyone in Oregon and the United States. The experience of other wealthy countries shows that this can be done in at least three ways (see also a the Princeton Public Health Review’s overview of health care systems):
With a National Health Insurance model, also called a single payer system or Medicare for All, where a single, usually public payer reimburses providers for all medically necessary care, and the providers may be independent private or public entities.
With a multi-payer system that has very tight government regulation and a mandate that everyone buys health insurance (Bismarck model), with sufficient public assistance so that everyone can afford to do so.
With socialized medicine (Beveridge model), where the government employs nearly all of the providers. This is also a single payer system, but we, and most advocates in this country, tend to use single payer to mean a system with a substantial portion of healthcare being privately delivered.
Of course no country has a system that can be classified entirely as one of these three options. The largest fraction of healthcare expenditures that are actually paid by a single entity in any one country is 85%, so no nation has a “true” single payer system. This can happen because a system is not that comprehensive (so some medically necessary services are not covered) or because people can opt to seek care from providers who do not get reimbursed by the “single” payer.
Many countries come close enough to one of these three options that they are generally classified as that sort of system, but a number of countries are usually classified as having a two-tier system (e.g. France, the Netherlands, Australia). The only economically developed country that is usually considered to have “socialized medicine” is the United Kingdom, but in all developed countries, including the United States, the government employs some healthcare providers, and all have some publicly funded hospitals, so all have “socialized medicine” to some extent.

We, along with most advocates in the U.S., are choosing to push for a single payer system.
A single payer system at the national level is often called Medicare for All because traditional Medicare in the U.S. has some aspects of a single payer system – there is only a single payer for traditional Medicare (Medicare Advantage complicates things) – though providers serve those who are covered in some other manner or are not covered at all, leading to excessive administrative costs in provider offices. Medicare is not universal – most people in the U.S. are not eligible for its benefits – so the modifier “for All” is necessary. Medicare is also not comprehensive, and has some other problems, so many advocates prefer to say National Improved Medicare for All (NIMA).
A well-designed single payer system would be:
Affordable
Savings will result from substantial administrative simplification in provider offices as well as on the payer side, from monopsony power (one buyer can get better prices from providers), and fraud reduction. Over the long term, preventive care and less stress will likely result in financial savings due to better population health. To put a number on the administrative savings, the RAND Corporation did a study funded by the Oregon legislature (see p. 101) in which they referenced a work that calculated the average estimates of economic studies of a national single payer system – the estimate is that administrative savings alone would result in 11% lower expenditures, saving $334 billion nationwide in 2016.
Universal
There will be no one who will have financial barriers to care, which is also an affordability and equity issue. There will be no underinsured or uninsured residents.
Equitable
Providers will have no financial incentive to treat some patients rather than others. All residents would be able to get the care they need when they need it, with no payments due based on the care they receive. Payments would be based primarily on income and/or wealth, and would occur at tax time, not at the time of care.
Comprehensive
All medically necessary services will be covered, including those related to the head – dental, vision, hearing, mental, and behavioral health.

The Arguments
The HCAO website features a variety of videos that explain why single payer is the answer.
Physicians for a National Health Program (PNHP) explains why the US needs a single payer health system.
Cornell Economics professor Robert Frank makes the economic case for single payer.
Mark Dudzic makes a labor argument for single payer.
Health Care for All - California makes a particularly compelling case for why we need single payer.
Why not keep our current system in the United States?
The short answer is that the U.S. system is not equitable, nor affordable, nor universal, nor comprehensive.
Not Equitable
Because there are financial barriers to care, some are uninsured, more are underinsured, and even when insured, those of lower income tend to have a greater difficulty getting appropriate care, the U.S. system is clearly inequitable.

Not Affordable
The U.S. spends much more per person on health care than any other country by any measure and the disparity is growing (see the evidence laid out in charts here). The essence of affordable health are is that no one would have financial barriers to care. In the U.S. It is estimated that 28% (41 million) of those aged 19 to 64 are underinsured, meaning they have financial barriers to care (see some statistics from The Motley Fool here).
Not Universal
We believe that everyone should be able to get the health care they need when they need it. Adequate health care should be treated as a public good or a fundamental or human right. In the words of the International Declaration of Human Rights (from Article 25) – “Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services …” All other wealthy countries have a universal system.
In the U.S., because some are uninsured (a number has been growing over the last two years due to federal efforts to hobble the Affordable Care Act) our system is clearly not universal.

Not Comprehensive
Even public insurance programs such as Medicaid and Medicare do not cover medically necessary services that are proven to be cost-effective. Too often, private insurance makes it difficult for providers to get reimbursed for medically necessary services. This happens even though the plan nominally covers such services.
For more information, see “Yeah, There’s a Problem” on the HCAO website.
Why Not Socialized Medicine?
The National Health Service in the United Kingdom (UK) and the Veterans Health Administration (VHA) in the U.S. are among the best examples of socialized medicine in wealthy countries. Both of these systems have higher satisfaction among users than nearly any other system (see the last row of a chart on p. 8 of International Profiles of Health Cares Systems, 2013 & VA Care Among Highest in Patient Satisfaction), though both are chronically underfunded, so dissatisfaction is much greater than it should be. While socialized medicine may indeed be the best system, most advocates believe that it will be more difficult and disruptive to shift the U.S. system to socialized medicine than it will be to shift to single payer. The advantages do not appear to be worth the potential extra disruption and difficulty.

Single payer advocates usually want to keep the VHA as an option for those who are eligible, since, when services are provided, it does a very good job of caring for people who have among the greatest need for medical care. The intent is that those eligible for VHA benefits could opt to get services within the single payer system when they so choose.
A difficulty with any reform is that even single payer is demonized as “socialized medicine,” an effort with a long and sordid history (see Chicago Magazine’s “How the AMA Scared Us Away From Socialized Medicine” and The New Yorker’s “The Lie-Factory”). “The Lie Factory” tells the story of the first real political consulting firm (Campaigns Inc., founded and run by operated by Leone Baxter and Clem Whitaker), with the interesting observation that:
Political consulting is often thought of as an offshoot of the advertising industry, but closer to the truth is that the advertising industry began as a form of political consulting
However, arguments calling every reasonable reform that involves the government playing some role “socialized medicine” is losing its effectiveness.
Why not a tightly regulated multi-payer (Bismarck) system?
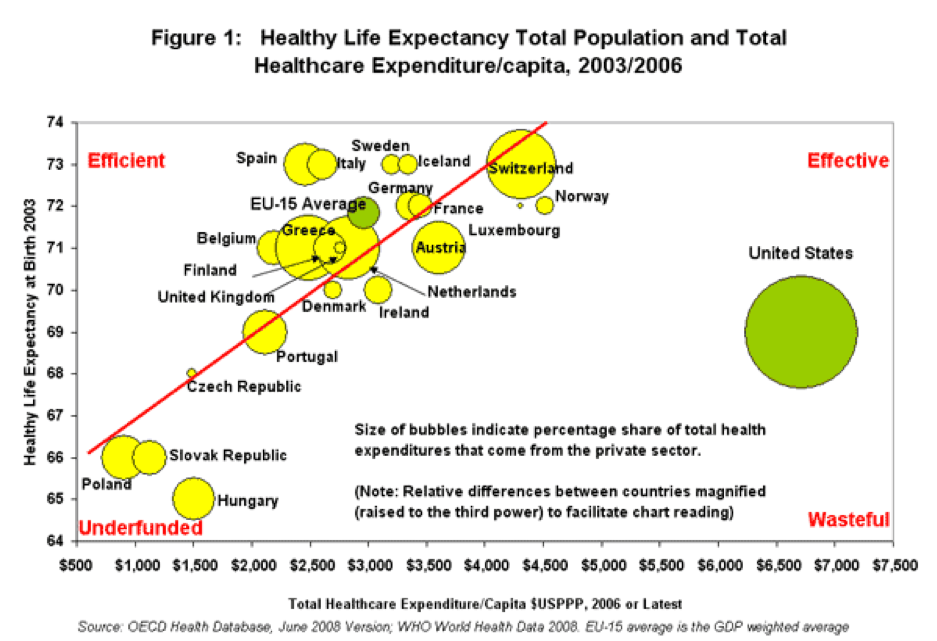
While a universal system that is not single payer nor socialized medicine (a Bismarck system, such as in Germany or Switzerland) can work well, there is a greater tendency towards inequities than with other universal systems. Such systems also tend to be administratively more complex and thus more expensive. Switzerland has the second most expensive health care system, and the German system is more expensive than most. German doctors face the 2nd most hassles with getting prescriptions authorized after the U.S., and they are the 2nd most unhappy doctors after the U.S. On average, Bismarck systems seem to cost about 25% more per capita than single payer systems (combining data from https://truecostblog.com/2009/08/09/countries-with-universal-healthcare-by-date/ and https://en.wikipedia.org/wiki/List_of_countries_by_total_health_expenditure_per_capita).
The U.S. has a long history of regulatory capture, which tends to suggest that keeping an effective Bismarck system will be difficult. We also have a long history of activists pushing for a single payer system, so absent clear advantages of a Bismarck system, there is not a good reason to switch direction.
Why not a tWo-Tier System?
Systems that are sufficiently mixed that most would classify them as two-tier are nearly as economically efficient as single payer systems, but they tend to have greater inequities. In practice, every country has, in essence, something like a two-tier system, even the United Kingdom - since patients with enough wealth can pay for care outside of the National Health Service. Even if advocates aim to design a system that is the ideal of a Bismarck, Beveridge, or single payer system, it will almost surely come out as a two-tier system. In the U.S., the recently proposed H.R. 1384, which is nearly an ideal single payer system, has aspects of a two-tier system, because only a restricted group of people will be able to opt for care within either the VHS or IHS system.
To the extent that a system is designed to be a two-tier system, it is designed to be inequitable. There should be a good reason for allowing any particular inequity.